The Appleton Area School District met 09/13/2021. They spent about an hour reviewing the district’s new Covid Dashboard and receiving a Covid update from Appleton’s Interim Health Officer Sonja Jensen and local doctor and Appleton Board of Health member Dr. Lee Vogel.
Per Superintendent Judy Baseman, the new dashboard had been unveiled at 6pm that very evening. Its purpose was to increase the transparency and accuracy of daily counts of Covid-19 positive cases as well as quarantines of students and staff resulting from contact tracing conducted by AASD nurses. She noted that:
- A current positive case indicates that an individual has been tested and confirmed positive.
- The number of quarantines indicates only that an individual AASD student or staff member has been ordered to quarantine because they are a household member of a Covid-positive individuals who is either an AASD student or staff member.
- If a person currently in quarantine tests positive for Covid-19, they would be removed from the quarantine case count and added to the positive case count.
- Current positive cases will be removed as students and staff return to school or work.
- Other illnesses and absences are not documented within the dashboard.
- Data will be entered and updated by 6PM each school day Monday through Friday and all Covid-19 cases and quarantines that are confirmed over the weekend or holidays will be added on Monday or the next regular school day.
Julie King and Polly VandenBoogart then reviewed the dashboard with the Board. It’s pretty straight forward so you can just check it out here: http://www.aasd.k12.wi.us/district/21-22_school_year/covid-19_dashboard

As Julie noted, it is very different from last year’s dashboard. It’s sortable by school building and student level. It also includes historical data
Polly pointed out that there are different dashboards being used at different area school districts, and she wanted to make sure it was understood that AASD only listed as “quarantined” students and staff who are household members of AASD students/staff members who have tested positive for Covid. Some other area districts have a more expansive definition of quarantine and Appleton’s quarantine numbers may look disproportionately low compared to those other districts.
Polly also updated them briefly on the district’s testing plans. The district’s testing vendor has all the information they need and are working to get testing paperwork and the electronic consent form for families up and running. The vendor is applying a code to each of the district’s buildings and they hope to have that ready soon so that they can begin PCR testing symptomatic staff and students.
Board President Kay Eggert asked if parents would need to sign the form ahead of time for their student to be tested at school. She also wanted to know what the procedure was to test students as well as the turn-around time for test results.
Polly said that AASD will not be conducting any of the tests, instead it will all be done by their testing service which was provided by the Department of Health Services. The district will have records of who has signed the electronic consent form. The vendor will communicate with the district and then Polly will then check the consent records and notify the vendor of who can and cannot be tested.
If a student starts to have symptoms during the school day, before that student goes home, the school would call the testing vendor who will be housed in a central location within the district and they will run someone over to that building to do a PCR test. That student will then go home, and the test will be sent to a lab in Milwaukee. They were hopeful they will get the results back in 24-48 hours.
She said the district was also going to provide a drive-thru testing opportunity for staff and some of the 4K families, and added that this PCR testing was for symptomatic staff and students only.
Board member Kris Sauter asked if a student needed to have a certain number of symptoms.
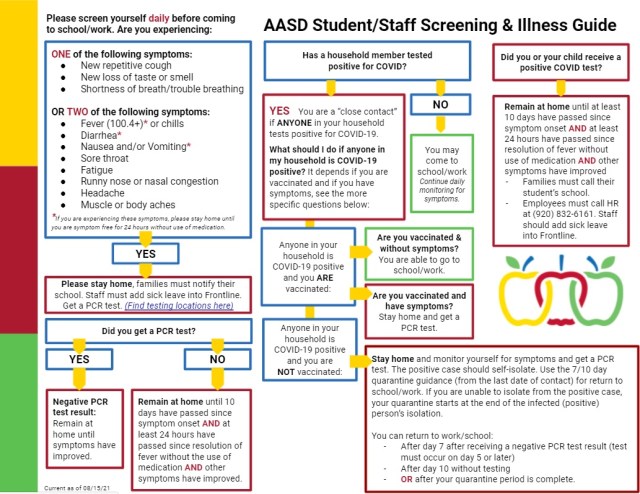
Polly said the main symptoms were (1) a new, repetitive cough, (2) new loss of taste or smell, and (3) shortness of breath/trouble breathing. If they have one of those the district would ask them to stay home. Otherwise, they would need to have two from another the secondary list of symptoms on the district screening guide. Students and staff were asked to follow the flow chart.
Board member Ed Ruffolo, said some districts in the US were looking at a test and stay approach as opposed to quarantining as a way to maximize in-person instructional hours. He understood that required the rapid test rather than the PCR test. A student with symptoms would have to keep testing negative every day in order to be allowed to stay in school. Then if they tested positive, they would need to follow that up with a PCR rest and quarantine. He asked about the wisdom of that approach and the ability to do it.
Polly said their testing vendor was willing to do that as well. They have multiple options available and want to meet AASD’s needs. They decided to start with the PCR symptomatic testing because that’s what the district’s protocol requires to return to school or work. They also decided not to do the rapid testing because they did antigen testing last year and didn’t feel like the response rate that received warranted continuing to do it. It is, however, something that they can ask their vendor to add at any time.
Ed encouraged them to consider that because it has a lot of advantages.
Kris asked how notifications worked [She asked this later on in the meeting, but I think it’s a little clearer and more relevant to move that discussion here in the recap.]
Polly said that, prior to the dashboard, families were notified via email regarding cases, but now the district was asking families to monitor the dashboard to help them determine if they felt safe sending their children to school. They will not be sending out notifications.
Kris asked if the dashboard indicated cases by classroom.
Polly said it does not. That was one of the challenges that school nurses faced with the previous system. Some families had multiple students in one school but due to confidentiality issues the notification emails didn’t indicate the classroom a covid-positive student had been in. Likewise, the current dashboard does not break things down to the classroom level. They were trying to balance that confidentiality with getting timely information out to families before the next school day.
After the Dashboard presentation, the Board moved on to the presentation from Interim Health Officer Sonja Jensen and Dr. Lee Vogel in which they shared some update on Covid-19 and research that was out there.
Interim Health Officer Jensen, talked about current case counts in the community. Between August 25 and September 7 there were 87 cases in children 17 and under in Appleton. During the 2-week period from August 18-August 31, there were 72 cases. During the two-week time frame before that (08/11-08/24) there were 59 cases, and between 08/04/-08/17 there were 59. She said that when they calculate the burden per 100,000 based on the population of that particular age group [she never said what Appleton’s population of people 17 and under is] they end up with a burden rate of 511 which was “very high”. This was slightly higher than for the overall population but otherwise pretty close.
Dr. Vogel said that adjusting the burden rate for 100,000 people was the easiest way to compare different groups. Back in the summer they felt comfortable allowing masks to be optional and at that time the 2-week burden rate for those under 18 ranged from 6-17 compared to the last couple weeks of 421 and 511. The current percentage of students at AASD with a positive case was 0.18% which translated into 180 positive cases out of 100,000 students. She concluded by saying, “So, I think masking is protective; the next few weeks will be telling.”
Interim Health Officer Jensen thanked her for that perspective and said that there had been a two-week period in June where there had been no cases in that 0–17-year-old age group, so it had changed a lot since then.
She reviewed the vaccination rates.
- State-wide, fully vaccinated – 52.4%.
- Outagamie county, fully vaccinated – 52.9%
- Appleton, fully vaccinated – 56.3%
- Appleton, fully vaccinated among the vaccine eligible population – 66.8%. She said that had gone up about 1 percentage point in two weeks.
Of Appleton’s 12–17-year-old population
- 49.6% are fully vaccinated (up about 3% from 2 weeks ago)
- 57.9% have at least one dose
Board member Amanda Stuck asked what the rate per 100,000 would be for them to start looking at taking masks off and for how long the rate would have to stay at that level before they could consider taking masks off.
Interim Health Officer Jensen said that the City of Appleton has followed the CDC recommendations and guidance which recommends that anyone in a community experiencing substantial or high rates of transmission should wear a mask in indoor public spaces whether or not they are vaccinated. “But right now, what the CDC says for schools—and I’m not saying this is what somebody needs to follow—but they recommend universal masking right now regardless of vaccination status and regardless of community levels of transmission.” [So, if the AASD is really serious about only following CDC guidelines, it seems that there is no situation in which they would make masks optional unless or until the CDC changes its guidelines.]
Dr. Vogel gave a fairly extended speech. I don’t want to misrepresent anything she said so I’ve just transcribed it, though I did remove some of the ums, uhs, and stutters.
“And I think for continuity to think about where that’s coming from right now is because the nation itself is in an upsurge of Covid activity relative to the Delta variant which is in every state and accounts for about, depending upon where you are, anywhere between 88 and 90-some percent of the activity right now. So, we’re in an upward phase and so there’s caution there.
“I think it’s probably worthwhile for me to talk a little bit about the context of the community because children are in families, families are in community, and our community is experiencing what it is experiencing. And one of the best, you know, registers or barometers of that is actually what’s happening in our health systems, clinics, and hospitals, and I’m gonna try to briefly talk a little bit about the quantitative data relative to that and then the qualitative data to that.
“When we look at just data as of September 8th for the Fox Valley region and I realize it’s very difficult to get just the municipal data alone but that’s where the qualitative will be helpful to you. We have about 92% of hospital beds in our area hospitals occupied and growing in there—in being occupied. We have about 9—88 almost 89% of our ICUs in the area hospitals occupied and while we have a, you know, hospital med surg units in peak capacity of only of about 53.8% let me translate that into what happened this last weekend with our two area–our three area hospitals. Based on experience of physicians and my colleagues involved. We’ve now had a couple of weekends and weeks where we have days where patients are being overnighted or stayed longer for up to 12 hours or more in the emergency room awaiting a bed availability, including an ICU bed. We have situations where doctors are calling around to 9 different hospitals to find an ICU bed for a diabetic who doesn’t have Covid but needs critical care. We have—part of that is a—and a lot of it actually is staff shortages. We have a nation-wide and a local staffing shortage for nurses, certified nursing assistants, RNs, and part of that is pre-covid, we had that. And Covid has not helped, certainly, because we really have staff that are really exhausted. We have one hospital that’s having the greatest difficulty is with nursing staff, another hospital where the difficulty is with doctors and hospitalists, and are activating actually their backup.
“This is actually considered almost peak activity in terms of hospitalization rates and ICU rates and it’s comparable with only about 1/3 of the case positivity rate currently now in our community compared with what the case positivity rate was at the peak of Covid during the winter time. We only have 1/3 of that activity, but we have the same amount of hospitalized patie—persons and ICU need and—In terms of how filled we are, as we were at that peak.
“And what’s the difference? For one thing, we are—instead of seeing our elderly who, unfortunately, when they were hospitalized in the middle of the winter time, were not vaccinated and not well and didn’t have the same reserve in their hospital stays were shorter, and we had a much higher death rate. Now one hospital is seeing—saying largely they’re admissions and their ICUs are full of persons who are 20-50 years old, and the other one’s seeing people who are 30-60 years old. And their length of stay, instead of being 5-7 days, maybe 12, is 20 to 30 days, and they’re fighting really pretty hard to make it.”
[I would have appreciated it if she had given some hard numbers. Yes, absolutely, our hospitals seem to be close to capacity right now, but it’s not clear just looking at the numbers on the WHA.org website that those capacity issues are being driven by Covid. As of 09/15/2021 across all 13 of the hospitals in the Fox Valley HERC area, we have 84 total people hospitalized with Covid. 16 of those are in the ICU. There are 104 ICU beds total and 694 other beds. Covid patients account for 15.4% of the ICU beds and 9.9% of the other beds. It would also be nice if, instead of making statements such as “their ICUs are full of persons who are 20-50 years old”, she could have just given some more definite figures because a span of 30 years is a pretty wide range and it would be nice to get some less vague numbers, likewise for the length of hospital stays. It’s easy to point to one 30-day hospital stay but is that actually common? It really bothers me when officials throw out general numbers that the public can’t review. At any rate, she continued…]

“So, what does that have to do with pediatrics? Well, because children live in families, and families live in communities, and it’s a community problem we need to try to do our best to reduce any sort of spreading of this disease that we possibly can. We actually have very good data to show that children actually do contract Covid. In the early Covid days we didn’t think that that was the case as much, but we also had a lot of communities that were shut down. We had schools that were shut down, and we just didn’t see quite the activity. Now we know it’s there.
“Childhood cases cumulatively over this time since Covid began represent about 15% of all cases, but when you look at the cases just in the last month, they now represent about 25% of cases. We have in our own community, there’s about 7% of all pediatric clinic visits are due to Covid and the current hospitalizations of children in our hospitals at Children’s in Neenah, at Saint Elizabeth’s Hospital, about 32% of children who are in the hospital are actually isolated either because of a combination of Covid or RSV which is uncharacteristically showing itself now instead of in the winter and is a serious childhood illness, and other viruses. And our kids are getting sicker and we’re seeing that rate increase. Used to be that about 0.1 to 1.9% of all childhood cases resulted in hospitalization and more lately it’s about 4% of Covid. So, we’ve got good reason to do the wise things that Appleton Area School District administration and our Board have done in terms of the masking.”
[Here again, I would have appreciated some more definite figures. I’m curious if the 7% of clinic visits are due to actual problems or simply diagnostic in nature. I would also have appreciated a clearer delineation between what the RSV rates are vs the Covid rate. She kind of blended them together and it wasn’t clear which one was the problem. She continued…]
“Just to talk about a little more overall effectiveness, ’cause there’s always questions. You don’t want to submit anybody to even a minor inconvenience and parents and community members and teachers and administrators alike. Doctors, we’re all asking ourselves: is it a minor inconvenience for children and what is it doing? But first let’s say if we’re gonna ask them to do that, is it effective? And we have a number of different ways of knowing whether that’s effective or not. Some of it is just what we call epidemiologic studies when we’re looking at situations where we have communities where there are schools that had masking and schools that didn’t have masking over the last year and we can see multiple studies that demonstrate clear differences in the rates of, of, um Covid. we have outbreaks in, in, in schools that have been looked at. Probably the biggest study in schools was done by Dr. Danny Benjamin, Duke University pediatrician and professor who in North Carolina looked at 11 districts, a total of a million children, and looked at the difference in the rates of contracting SARS—or the Covid-19—and found clear differences between the schools that and districts that used mandatory masking compared with those that didn’t have mandatory masking. And this is really pretty helpful to know.”
[Note: as far as I can tell, the study she is referencing did not study transmission rates in masked vs unmasked schools in North Carolina. In their New York Times opinion piece, the study authors themselves very clearly state, “Because North Carolina had a mask mandate for all K-12 schools, we could not compare masked schools to unmasked schools. To understand the preventive impact masks can have, we looked outside North Carolina for comparisons. Data from our research and from studies conducted in Utah, Missouri and Wisconsin shows that school transmission rates of coronavirus were low when schools enforced mask mandates. By contrast, one school in Israel without a mask mandate or proper social distancing protocols reported an outbreak of Covid-19 involving 153 students and 25 staff members.” So, essentially, they studied transmission rates in fully vaccinated schools in North Carolina and did not have any un-masked schools to use as control groups. Rather, they compared the data they gathered from the North Carolina schools to data from other studies that they themselves had not conducted and which did not necessarily utilize the same research methodology they had for their study. At any rate, Dr. Vogel continued…]
“There was a recent study in Bangladesh which is also the first randomized control trial—you know, we haven’t been randomizing people to have Covid or not have Covid—but we now have…uh 600 villages in Bangladesh–a really nicely done study that looks at those villages that were actually randomized and taught and encouraged to use masks compared with those that weren’t and for a 29% increase in mask rate in the cont—uh, the masked villages compared with the unmasked—there was a 9% reduction in Covid. And that’s without full universal masking.
“So, then the question is ‘is masking safe’? You know we all, when we wear masks, we become periodically uncomfortable, where we’re feeling hot, sometimes we feel like maybe we can’t breathe as well. The studies have been done looking at oxygen and carbon dioxide–these are molecules that go through masks and exchange. And there are no differences in our oxygenation or our blood’s ability to get rid of the—or our breathing ability to get rid of the carbon dioxide. And some of those studies have also been done in fairly serious adults with serious lung diseases like emphysema. We may feel hot from time to time, but we usually do well.
“Remember that our children were masked when they came back to school last school year until the end of the school year, and they did remarkably well, and in these first few weeks we’re hearing parents and teachers be noting real positivity. Kids get it and they can do it. There’s been some recent studies thanks to our pediatricians who are on it—our expert pediatricians around the country, particularly at children’s hospitals—and they’re actually looking at studies. They’re looking to see does masking—and there are some previous studies to indicate this—that masking doesn’t harm a child’s ability to interpret language, to learn language, um, and it doesn’t impede cognitive abilities. So that’s really, that’s really pretty good news.
“So, I think that’s kind of my take on things that I wanted to present and then if I could answer any questions. I will answer questions. And sometimes I’ll say I don’t know and I’ll get the information because I think there’s one thing to–that we all are aware of is that nobody gave us a playbook for a pandemic. We don’t have data from the prior pandemic, right? We’re mostly going through this and learning as we go along; we’ve got people dedicated to finding out.”
Board member Jim Bowman said there seemed to be great data on the effect of vaccines on infections, and he knew that if he was vaccinated, he was much less likely to be infected with the Delta variant or to have adverse health outcomes if he did get infected. But he hadn’t seen good data on the effect of vaccination on transmission. Was there a difference in the rate of transmission from vaccinated people vs unvaccinated people?
Dr. Vogel said that gathering the data on virus transmission in vaccinated groups is something that’s ongoing and in progress. In general, the Delta variant is about 200% more transmittable than previous variants which was probable due to the much higher viral load it creates. She said they do know that vaccinated individuals even in all-vaccinated events will spread the disease. On the east coast there was one big super-spreader event that was an all or mostly vaccinated event.”
[She may have been referencing the breakthrough outbreaks in Barnstable County, MA.]
“Regarding wearing masks, healthcare system studies have indicated that the breakthrough rate for vaccinated people in that group is less than 1%, which suggests that the masks are working there. She said there is data that shows vaccinated people can spread it. But vaccinated people are getting milder symptoms and usually not getting sick enough to be hospitalized or require ICU care.
Board member Deb Truyman asked how they know that it’s safer to wear a mask incorrectly than not wear one at all. She thought a lot of kids at school were probably fidgeting with their masks and not wearing them correctly.
Doctor Vogel answered, “I guess I would say that, you know, in the realm of both adults and children, we’re gonna have some that wear it incorrectly. And I think we should assume that children are children everywhere. So, if we’ve got school districts and we’ve got a study in North Carolina with a million children and eleven different districts and those that are universal masking compared with those that aren’t universal masking–those universal masking school districts have schools with the same kinds of kids that we have. Some of them are wearing them incorrectly, and we’re reminding them and they’re fidgety and all of that. But even with all that potential flaw of less than perfect wearing of the masks, there’s a real difference in the spread and the occurrence of Covid in those children. So, we infer it, and we accept it because it certainly is better than no mask or optional masking.” [Again, this study she is referencing did not do a one-to-one comparison of masked schools to unmasked schools in North Carolina and it’s not clear that the un-masked schools in the other studies that the North Carolina study drew on for comparison utilized the same non-masking mitigation strategies AASD is using or that the North Carolina schools are using. In fact, the study authors clearly stated that the Israeli school in a study they used for comparison did not utilize “proper social distancing protocols.”]
Deb asked if they knew what other mitigation strategies were used at those North Carolina schools. She firmly believed that AASD has a strong number of effective mitigation strategies in place and wondered if masking was doing any good if students were wearing those masks incorrectly. “I don’t want to infer. I don’t want to infer anymore with the health of our children and their effect on learning. I would like to see evidence.”
Dr. Vogel said that masking is one of the strongest approaches and the reason the CDC recommends masking and recommends a layered approach is that when removing masking impacts some of the ability to reduce spread. She said the mitigation measures that North Carolina used were quite similar to AASD’s in terms of social distancing, hand washing, and improved ventilation. The difference was that in the school districts that didn’t use masking, they were also using some of the other things, but masking really was far above and additive to the other measures that we use. “And I don’t think that that’s an inference; I think that’s pretty good data that’s guiding us.”
Deb asked, “Where is the studies? Where is the evidence?”
Dr. Vogel answered, “I would be glad to summarize it and send it.”
Ed referred back to Amanda’s question earlier. At some point they were going to have to make a decision about when it will be appropriate to unwind some of their mitigation strategies–masks being one of the more controversial ones. He knew they couldn’t give the Board a magic number but he wondered what the Board should be looking at to guide their decisions. They’ve talked about vaccination rates, burden rates, and community transmission. He wanted to be able to make evidence-based decisions, understanding that there would be people who would disagree regardless of what they decide. What could the Board as lay-people look to one-to-one really understand when it would safe to take the masks off and when there would be a high likelihood that the masks would stay off.
Dr. Vogel answered, “I think I’m gonna preface this by honestly saying I appreciate that you know that I don’t have a crystal ball, and I will say that I do look to the CDC for guidance as they gather and accumulate and assemble the kind of evidence in sort of a moving trajectory, as you will. I do know that they–while they have a recommendation in communities where there’s substantially transmissible burdens and rates to continue to be masking, and I believe that previously less than 100 per 100,000–but I will have to look that up. To give you a little better idea though in terms of how long. The modelling that’s been done for the Fox Valley area looking at the Delta Variant and–that’s the other thing, it’s a wild card, right? It’s different, but when they factor in how the Delta Variant has acted in other countries and other states and when it’s peaked and when it’s started to come down and tried to do some predicting and some modelling, it looks like we may peak–if we’re lucky–we may peak in anywhere between two to four weeks and then start coming down the mountain on the other side. And so how far down the mountain we have to get is something we need to kind of look at and that may change based on CDC guidance, but I hope that helps a little bit.”
Ed thanked her and said he had read that Pfizer will be requesting FDA approval to provide vaccinations for younger children and those might be available by Halloween. What impact did Dr. Vogel think that would have on AASD’s mitigation strategies?
Dr. Vogel responded, “I think it’s huge.” She said that experts argued whether herd immunity would be reached once 75% of the population was vaccinated or 85%. She thought more toward 85% was better. the more it’s 85% the better. She thought vaccination was the key. The reason why we haven’t had to wear masks or gloves to protect our children from common childhood diseases is because they’ve been immunized against those illnesses. She thought that vaccination was “the biggest prevention and it’s the cure.”
She said they were all waiting for those vaccinations to come out for the children and the community could be helpful about it. “The more positive we can be about embracing vaccines and the sooner for our adult populations too–particularly the 18–24-year-old group appears to be some of the most reluctant–and if we can have conversations with our doctors and feel more comfortable this is a really incredibly well studied vaccine and very safe vaccine. Because the longer it goes on that we don’t have a vaccinated population, the longer the virus percolates in those, in unvaccinated people, the more it has a chance to develop into something that won’t respond to our vaccine. So, it’s a race, but hopefully we’re winning it.”
Ed said, “Since the 23rd I’ve been very conscious about wearing my mask everywhere I go because I voted for it, I should follow it, and I’m very concerned when I go out in the community that it’s a little lonely out there for us mask-wearers. There’s a lot of people in grocery stores, in restaurants, sporting events that have chosen not to wear a mask, and of course we can’t control that. How much negative impact is that having on our mitigation strategies, requiring to wear a mask while in school, and what other things can we do to help counterbalance that?”
Dr. Vogel answered, “I don’t mind saying that the rise of the slope of the Delta virus positivity in our community is directly related to people who are out and about contacting other human beings’ breathing space without a mask. It just is.”
[I don’t know what she based that statement on. We had a similar increase during this time last year even though, starting August 1, 2020 we had near universal masking in public places.]


“We see this bump. We see the bump with unmasked people after the 4th of July, and then you get EAA and then you get Mile of Music where everybody had to go indoors because it rained and many people weren’t masked and then you get–and then you get Labor Day and–and thank goodness if we’ve got masked children we’re not asking and now they’re back to school because they’re masking and so that’s helpful. But, yeah, it’s very harmful.”
Interim Health Officer Jensen said, “I would agree, and I would say by wearing your mask–even though you feel a little lonely–I mean, the more that you do it and the more that we are role models for others in the community and want to protect others then, hopefully, it will catch on again.”
Deb said she had seen some slides from the CDC that suggested masks trap particles of virus and the mask wearer then rebreathes those particles. She wondered if wearing a mask while sick could cause someone to get a worse case of covid.
Dr. Vogel said that was an excellent question. “My sense is from knowing how viruses replicate that what’s happening in your mucus membranes already far, far outweighs any sort of potential rebreathing. And remember, it’s trapped so it’s trapped there between the layers.” She said she would research a little more for a fuller answer.
Ed asked if there was anything else AASD should be doing in terms of mitigation strategies to help prevent the spread of covid within its schools and maximize the students’ opportunities to have in person instruction.
There was another very long pause before Dr. Vogel responded that everyone was trying to get a handle on the best testing strategy. The sooner one could identify a symptomatic child and the shorter the turnaround for test results, the better. There were expenses and practical issues related to that, however. She noted that there is a covid testing reagent shortage in the nation.
She also thought that everyone was still trying to figure out the right strategy for quarantining in relation to school systems. School systems were all doing different things in terms of who qualified as a close contact beyond household members. She thought the intent of the administration and public health department was to keep up a good dialogue and see if they needed to change their strategy. She thought the school was looking at smaller classes and has used pods to minimize contact. One strategy was simply constant communication, trying to stay ahead of the research, and to have a good dialogue.
View full meeting video here: https://www.youtube.com/watch?v=zfIT4Xx18xY
View full meeting agenda and documents here: http://go.boarddocs.com/wi/aasd/Board.nsf/goto?open&id=C6F2ZJ62B16D
Be the first to reply